Perceptions of Measles and vaccine Knowledge and Hesitancy among Health-care students in an Albanian University: results from a survey
Gjini E.,1 Cenko F.,2 Moramarco S.,3 Biondi G.,4 Agosti G.,4 Mehmeti I.,3 Buonomo E.3
1 Department of Biomedicine, Catholic University “Our Lady of Good Counsel”, Tirana, Albania
2 Department of Medical Sciences, Catholic University “Our Lady of Good Counsel”, Tirana, Albania
3 Department of Pharmaceutical Science, Catholic University “Our Lady of Good Counsel”, Tirana, Albania
4 Department of Biomedicine and Prevention, University of Rome Tor Vergata, Rome, Italy
5 School of Hygiene and Preventive Medicine, University of Rome Tor Vergata, Rome, Italy
Introduction
Measles is a highly contagious vaccine-preventable disease with serious complications such as pneumonia, croup, encephalitis and death. Before the vaccine introduction, more than 30 million cases and more than 2 million deaths were occurring globally each year.1 The World Health Organization (WHO) set the year 2020 as a target date for the eradication of measles in Europe,2,3 where the prevalence is at its highest rate in a decade: 82,596 people were infected and 72 died from the preventable disease during 2018.4 Preliminary data shows that cases rose by 300 percent globally in the first three months of 2019, compared to the same period in 2018.2 WHO recommends immunization for all susceptible children and adults for whom measles vaccination is not contraindicated. Covering all children with two doses of measles vaccine, either than alone or in a measles-rubella (MR) or measles-mumps-rubella (MMR) combination, is considered as a standard for all national immunization programs.5
Albania is one of the countries in the WHO European Region that have successfully interrupted endemic transmission of measles and rubella. Since achieving measles elimination in 2015, the country has reported sporadic imported cases of measles. This includes cases in the second half of 2017 that were followed by a few separate outbreaks with a small number of cases and a limited period of transmission. In 2018, 1,466 cases were recorded, while from January to August 2019 measles cases were 481 with 2 deaths.6
In Albania, measles vaccine has been in systematic use since 1971 as a single antigen. The routine mandatory vaccination against measles was introduced in the national immunization calendar for all new birth cohorts. The introduction of bi-vaccine of measles and rubella in October 2000 was combined with a catch-up campaign covering all children from 1 to 15 years old. Since then the measles vaccine in the calendar of mandatory immunization is scheduled with a basal dose at the age of 12 months and the booster dose at the age of 5 years. The mumps antigen was added to the National Immunization Program since the January 2005 introducing the combined tri-vaccine MMR, which is still in use today in Albania.7
In Albania measles vaccination is part of the vaccines that are mandatory for Health Care Workers (HCWs).8 The literature data reports that HCWs are more likely to develop measles infection than general population (from 2 to 19 times).9,10 They are potentially exposed every day to biological risks, working with infectious patients and coming into contact with contaminated fluids and materials. Furthermore, the vaccine may protect not only the HCWs but may also avoid the spread of the disease to susceptible populations (i.e. the patients).
The knowledge, behaviors and attitudes of HCWs regarding vaccinations can influence patients’ decision-making processes.11 Misinformed personnel may be a barrier to acquiring high vaccination coverage within a population: patients trust in their HCP HCWs is often associated with their ultimate decision whether to accept or decline vaccines.12,13 Additionally, the WHO Strategic Advisory Group of Experts (SAGE) on Immunization has recognized vaccine hesitancy as a growing problem and has aimed one of the most impact determinants to the beliefs and attitudes of HCWs.14 Therefore, it is essential to ensure health care providers are aware of evidence, safety and efficacy of vaccines.11
Evaluation of the knowledge, perceptions and apprehensions of students enrolled in health care professions can help providing insight into how to improve and guide immunization training from the start of professional education. Research in this area is still lacking.
The objective of this study was to assess the vaccination attitude, knowledge, beliefs and vaccination status of health care students attending the first year of health care faculties at the Catholic University “Our Lady of Good Counsel” in Tirana, Albania.
Methods
The survey was conducted from January to February 2019, on the entire population of health care students attending the first year of different faculties of the Catholic University “Our Lady of Good Counsel”: Medicine, Pharmacy, Nursing, Odontology and Physiotherapy. An anonymous self-administered questionnaire was used, that was constructed after a literature review and using the findings of qualitative studies and empirical literature.15,16
The questionnaire collected information on: (i) demographic characteristics (sex, age and specialization); (ii) self-reported measles vaccination status; (iii) knowledge and perception on measles; (iv) beliefs in safety and efficacy of measles vaccine.
To evaluate the knowledge of perceived seriousness of measles, an overall score was generated for each respondent: 1 point was assigned for correct answers, 0 for uncorrected or not given answers. Score could reach a maximum of 7 points.
Beliefs in safety and efficacy of measles vaccine were assessed to investigate students’ hesitancy, since health care professionals often cite “safety concerns” as the most dominant reason for their self-vaccination hesitancy.17
Data were extracted and analyzed using SPSS v.26. Categorical and numerical variables were compared using chi-square and t-student tests respectively. Results were considered statistically significant at a p-value threshold <0.05.
Results
Characteristics of respondents
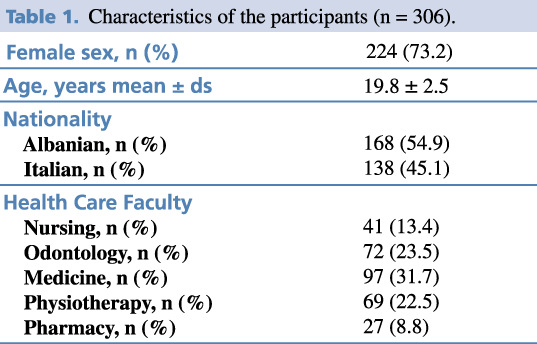
A total of 306 university students answered the questionnaire. Students from the faculty of Medicine had the largest representation in the sample, with 97 respondents in total (31.7%); Pharmacy had the fewest respondents, with 27 (8.8 %). The majority of respondents were female (71,2%), the mean age was 19.8 ± 2.5 SD. 54.7 % of respondents were Albanians (Table 1).
Table 1. Characteristics of the participants (n = 306).
Measles vaccination status of respondents
The vaccination status was assessed by the questionnaire-based confirmation of the respondent.
69% of respondents answered that they were vaccinated, with no significant differences between genders. Conversely, a significant difference in vaccination coverage between Italians and Albanians was found (52.8% Vs 47.2%; p<.0001).
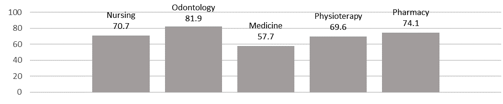
Figure 1 shows the percentages of positive answers on measles vaccination status according to different faculties: Medicine had the lowest percentage while Odontology had the highest one. The difference between the two values was statistically significant (57.7% vs 81.9%; p=.001).
Figure 1. Percentages of positive answers on measles vaccination status splitting by the faculties.
Knowledge and perceived seriousness of measles
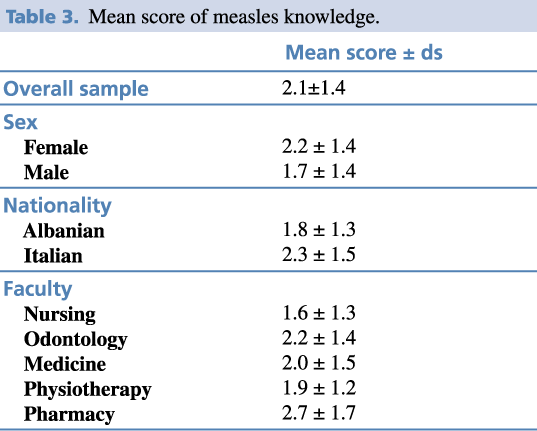
Table 2 shows answers on measles knowledge and perception, while Table 3 reported the score generated with the 306 students’ answers. The mean score was 2.1±1.4. No significant differences in relation to gender were found. Italian students had a higher knowledge of measles compared to Albanians (2.3 vs 1.8; p=.043).
In order to investigate whether the kind of faculty could influence the knowledge, the association between the score and the faculty was analyzed. A significant difference was found between the Nursing and Pharmacy students (1.6 vs 2.7 respectively; p=.022).
Table 2. Measles knowledge.

Table 3. Mean score of measles knowledge.
Vaccination Measles Hesitancy: belief in safety and efficacy of measles vaccine.
To investigated HCWs’ measles vaccine beliefs and hesitancy, three different questions were included in the questionnaire: (i) Is there a connection between autism and the measles vaccine? (ii) Does the measles vaccine pose a risk to my health? (iii) Will the measles vaccine protect my patients?
Students’ uncorrected answers are reported in Table 4.
Table 4. Percentages of mistakes on safety and efficiency of measles vaccine (Hesitancy).

No significant differences in relation to gender were found. Albanian students showed less trust in safety and efficiency of the measles vaccine (Table 5).
Table 5. Percentages of mistakes on safety and efficiency of measles vaccine by nationality.

Comparing measles vaccination status and the percentages of wrong answers, a higher risk of mistakes was found in students without measles vaccination for the second and the third questions,
OR: 3.9; IC 2.3-6.6; p<.000 and OR:5.2; IC 3,0-9.11; p<.0001 respectively.
Discussion
In literature, there is still a scarce research on knowledge, behaviors and perceptions of HCWs regarding vaccines, and when specifically considering Albania, this study is the first one curried out in a sample of health care university students in the country. Over results highlighted that only over half of our sample reported to be vaccinated for measles and in literature there were no more comforting results. In a study conducted in Lille, France, 78% of health care students reported to be covered for the measles vaccine.18 Similar coverage was found between medical students in The James Cook University in Australia.19 In 2019, an Italian study showed a low self-reported vaccination coverage for MMR, among physicians (42.9%) and nurses (58.3%).20 However, positive results were reported in another study conducted in France on medical residents of the University of Aix/Marseille, with higher coverage among residents of pediatrics, gynecology-obstetrics and medical specializations (≥95%).21
In addition, our findings demonstrated that students need to acquire knowledge and awareness on measles and other vaccine-preventable diseases. This is of paramount importance since it is well documented that the knowledge and attitudes of HCWs regarding vaccines can influence patients’ decision-making processes and misinformed personnel may produce a barrier to acquiring vaccination coverage within a population.12,13
Analyzing students’ scores, the results highlighted that they did not consider measles as a serious disease. Even another Italian study, conducted on healthcare workers, showed that only 45.5% of the sample gave a correct answer to the question: “Which infectious diseases could be a risk for my health, if I am not vaccinated?”, referring to the measles.15
About measles vaccine beliefs, more than 2/3 of the sample did not trust the safety and efficacy of the vaccinations.
In a study investigating the immunization knowledge, attitudes and practices among health professionals in Australia, similar results have been found analyzing the awareness about the association between MMR vaccination and chronic diseases, such as autism: only the 59% of health professionals knew that there was no association.22 Similar percentages were found for medical students’ in both a German and a Serbian study (55.8% and 53.4% respectively).23,24
Our findings could be proved by the susceptibility of medical students to false media allegations or improper education. Betsch et al. also observed a high prevalence of using e-health sources of information and concluded that early medicals education should prevent the students from using internet as an information source regarding vaccination.23
Lack of knowledge about vaccination among health professionals was specified as being linked to vaccine hesitancy in the population. Health professionals’ knowledge and attitudes about vaccines have been shown to be an important determinant of their own vaccine uptake, their intention to recommend vaccines to their patients as well as the vaccine uptake of their patients.25
In our sample, Albanian students had significant lower vaccination coverage and mean score and a higher lack of knowledge about measles vaccination than Italian ones partially due to their different public health vaccine policies. Significant differences in scores and mistakes on safety and efficiency of measles vaccine were found when comparing the Nursing’s and Pharmacy’s faculties. These differences could be explained by nationality, because of most of Nursing’s students were Albanians and most of students attending Pharmacy were Italians. These different results could be justified by divergent immunization policies and strategies in both countries.
Albania claimed to have successfully interrupted endemic transmission of measles and rubella in 2015 and it might cause a lowering in public attention on measles and a rise of misguided safety concerns regarding vaccination during the following years.26
An Albanian study about perceptions and knowledge of nurses about mandatory and recommended vaccinations reported that the barriers to HCW immunization included the fear to adverse events following immunization, the suspicion about the long-term effects on the health of vaccinations and the lack of knowledge of the nurses about vaccines recommended for HCW. No religious issues related to the barriers to immunization were reported.26
However, as limitations of the study, no information on socio-economic conditions, either on parental status and their literacy were conducted, therefore some bias could still be being identified.
Conclusion
This study highlighted that University health care students, at the beginning of their studies, did not consider measles as a serious disease and had misconceptions and hesitancy about measles’s vaccine safety and efficacy. This survey can be considered as a teachable moment on public health education of new health care students, in order to improve their professional knowledge. In this perspective, it is necessary to improve professional training with the aim of making a real change in behaviors, which would enable HCWs to counter Hesitancy and to play an important role in the future of public health. Further researches need to be conducted to evaluate the growing in knowledge on measles vaccination at the end of their academic courses, as well as the changes in perceptions and behaviours.
Limitations
Results of this study should be analyzed, considering that vaccination status relied on self-reported data rather than laboratory test results. Despite this potential bias, the findings of this study provide useful information about the need to improve HCW’s knowledge and to make them conscious of vaccine uptake.
References
- The Who. Weekly Epidemiological Record. No 17, 2017, 92, 205–228. 28 APRIL 2017, 92th YEAR
- World Health Organization. Immunization, Vaccines and Biologicals. Vaccine and Disease. Measles. https://www.who.int/immunization/diseases/measles/en.
- The World Health Organization. Emergencies Preparedness, Response. Measles – European Region. https://www.who.int/csr/don/06-may-2019-measles-euro/en.
- World Health Organization. Measles in Europe: Record Number of Both Sick and Immunized. Copenhagen, 7 February 2019.
- Expand Program on Immunization, IPH. National Vaccination Coverage Survey for All Antigens. 1995-2005
- World Health Organization. Regional Office for Europe. Albania Mounts Rapid and Comprehensive Response to Measles Outbreak.
- Kakarriqi E. Epidemiological Background of Infectious Diseases in Albania and Their Prevention and Control in the Context of Natural Disasters and Infectious Disease. 2002:20-27, 77-81.
- Maltezou HC, Botelho-Nevers E, Brantsæter AB, Carlsson RM, Heininger U, Hübschen JM et all. Vaccination of Healthcare Personnel in Europe: Update to Current Policies. Vaccine 37 (2019) 7576–7584.
- Fiebelkorn AP. A Global Perspective of Vaccination of Healthcare Personnel against Measles: Systematic Review”. Vaccine 32 (2014) 4823–4839.
- Maltezou H.C. Measles in Health Care Settings”. American Journal of Infection Control 41 (2013) 661-3.
- Sočan M, Erčulj V, Lajovic J. Knowledge and Attitudes on Pandemic and Seasonal Influenza Vaccination among Slovenian Physicians and Dentists. Eur J Public Health. 2013;23(1):92–97.
- Committee NVA. Assessing the State of Vaccine Confidence in the United States: Recommendations from the National Vaccine Advisory Committee: Approved by the National Vaccine Advisory Committee on June 10, 2015. Public Health Rep. 2015;130(6):573–95. Available from: https://www.ncbi.nlm. nih.gov/pmc/articles/PMC4612166/.
- Kasting ML, Wilson S, Dixon BE, Downs SM, Kulkarni A, Zimet GD. A Qualitative Study of Healthcare Provider Awareness and Informational Needs Regarding the Nine-Valent HPV Vaccine. Vaccine. 2016;34(11):1331–4.
- Dubé E, Gagnon D, Nickels E, Jeram S, Schuster M. Mapping Vaccine Hesitancy – Country-Specific Characteristics of a Global Phenomenon. Vaccine 2014;32(49):6649–54.
- La Torre G, Scalingi S,Garruto V, Siclari M, Chiarini M and Mannocci A. Knowledge, Attitude and Behaviours towards Recommended Vaccinations among Healthcare Workers. MDPI. 2017.
- Bolton-Maggsa D, Conrada D, Keenana A, Lamdenc K, Ghebreheweta S, Vivancosa R. Perceptions of Mumps and MMR Vaccination among University Students in England: An Online Survey. Vaccine. 2012.
- Yaqub O, Castle-Clarke S, Sevdalis N, Chataway J. Attitudes to Vaccination: A Critical Review. Social Science & Medicine. 2014
- Faure E, Cortot C, Gosset D, Cordonnier A, Deruelle P, Guery B. Vaccinal Status of Healthcare students in Lille. Statut vaccinal des étudiants en santé: l’expérience lilloise. Medicine et maladies infectieuses. 2013.
- Fergus E, Speare R and Heal C. Immunisation Rates of Medical Students at a Tropical Queensland University. Tropical Medicine and Infectious Disease. May 2018.
- Napolitano F, Bianco A, D’Alessandro A, Papadopoli R and Angelillo IF. Healthcare Workers’ Knowledge, Beliefs, and Coverage Regarding Vaccinations in Critical Care Units in Italy. Vaccine 37 (2019). 6900–6906.
- Korhonen T, Neveu A, Armengaud A, Six C, Danis K and Malfait P. Low Measles Vaccination Coverage among Medical Residents in Marseille, France: Reasons for Non-Vaccination, March 2013. European Journal of Public Health. 2015. Vol. 25, No. 3, 512–517
- Leask J, Quinn HE, Macartney K, Trent M, Massey P, Carr C, et al. Immunisation Attitudes, Knowledge and Practices of Health Professionals in Regional NSW. Aust N Z J Public Health 2008;32(3):224–9.
- Betsch C, Wicker S. E-health Use, Vaccination Knowledge and Perception of Own Risk: Drivers of Vaccination Uptake in Medical Students. Vaccine 2012;30(6):1143–8.
- Cvjetkovic SJ, Jeremic VL, Tiosavljevic DV. Knowledge and Attitudes toward Vaccination: A Survey of Serbian Students. J Infect Public Health. 2017;10(5):649–656. doi:10.1016/j.jiph.2017.05.008
- Dubé E, Gagnon D, Nickels E, Jeram S, Schuster M. Mapping Vaccine Hesitancy – Country-Specific Characteristics of a Global Phenomenon. Vaccine 2014; 32(49): 6649–54).
- Malorgio S, Mehmeti I, Cenko F, Giampa E, Talucci C. Perceptions and Knowledge of Albanian Nurses about Mandatory and Recommended Vaccinations for Healthcare Workers in Albania. Online publication ahead of print, AJMHS Vol 51, 2019.